Q: Do targeted toxin-treated cells die by apoptosis?
A: There are, allegedly, two ways for cells to die: by apoptosis or necrosis. According to Fiorenzo Stirpe (the discoverer of saporin), saporin-intoxicated cells die both ways, some by one, others by the other.
There is good literature that states that cells die by apoptosis. Saporin and apoptosis gives 25 hits in PubMed. For instance:
Bergamaschi G, Perfetti V, et al. (1996). Saporin, a ribosome-inactivating protein used to prepare immunotoxins, induces cell death via apoptosis. Brit J Haemat 93:789-794.
However, Seeger et al., did not find evidence of apoptosis in an electron microscopy study with cells dying from 192-IgG-SAP and concluded they die from necrosis. Saporin and necrosis gives 11 hits in PubMed.
One of the tests you can use to test your targeting agent for internalization is the in vitro Cytotoxicity Assay. Protocols to assist in preparing for, executing and interpreting results are now posted on our website.
There are several protocols available.
Preparing for a Cytotoxicity Assay using Secondary Conjugates. This protocol will be helpful when using our secondary antibody-saporin conjugates with your primary antibody. These include Anti-M-ZAP (Cat. #IT-30), Goat-ZAP (Cat. #IT-36), Hum-ZAP (Cat. #IT-22), Mab-ZAP (Cat. #IT-04), Rab-ZAP (Cat. #IT-05), and Rat-ZAP (Cat. #IT-26).
Preparing for a Cytotoxicity Assay using Streptavidin-ZAP. This protocol will be helpful when using our streptavidin-saporin conjugate (Streptavidin-ZAP, Cat. #IT-27) with your biotinylated targeting agent (peptide, ligand, cytokine, growth factor, antibody, etc.).
Concentration Calculation: Convert molarity to mg/ml and mg/ml to molarity. This protocol will help in determining the correct amount of material to use in your assay. There is also a link to an Online Calculator.
Cytotoxicity Assay for Targeted Toxins in vitro. This protocol includes photos of what your plates should look like during the assay process. It takes five days to complete this assay. Start on a Monday and develop on Friday. There are many factors that go into a successful cytotoxicity assay. This protocol should help you design and execute appropriately.
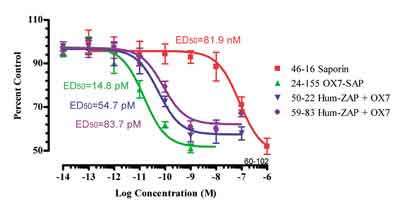
Preparing Cytotoxicity Data. This protocol will give an example of how to process the data from a Cytotoxicity Assay. ATS uses SOFTMax Pro software connected to a plate reader to determine the A490 value. Then we import this data into Prism software (GraphPad) to conduct further data analysis. Here is a figure generated with Prism.
We hope these protocols will be helpful to you in your research. If there are additional protocols or tutorials we can provide, please do not hesitate to ask.
This graph gives important information about how the potency of your targeted toxin. The ED50 is the Median Effective Dose (produces desired effect in 50% percent of population). The lower this number is, the more potent the targeted toxin.
Q: I have a question about what solutions might be incompatible with the conjugated saporins. We have done an experiment where we injected a mixture of saporin conjugate (same batch we’ve used in previous studies here) and a cocktail of 5,7-dihydroxytryptamine and 6-hydroxydopamine (in 0.1% ascorbic acid) to try to deplete multiple neurotransmitters.
The way we did this was to prepare both solutions at double strength and to mix them immediately before loading the syringe and placing the injections. So the final solution has 0.05% ascorbate, 0.01 mg/ml saporin conjugate, and I think 6 µg/µl 5,7-DHT and 4 mg/ml 6-OHDA.
Anyway, we are doing the histology now and the cholinergic lesion didn’t work. I’m wondering whether the ascorbic acid might have either damaged the conjugation of the saporin to the antibody, or have inactivated the saporin molecule itself somehow.
A: You have well-described what the problem is. A reducing agent will inactivate the toxin, and of course, ascorbic acid is a potent reducing agent. Because of your experience, we have added a line in the data sheet to caution people. This is the first report of this happening in nearly fourteen years of business, so it just had not been an issue.
Q: I’m using your secondary conjugate Mab-ZAP (Cat. #IT-04) and it’s not killing my cells. I’m not following the protocol on the data sheet. I’m doing flow cytometry. I have 70,000 cells per well. I mix Mab-ZAP with my primary antibody and add it. When I count the cells, there is no decrease. My cells grow very slowly. I didn’t see anything after 72 hours.
A: The protocol on the data sheet is described in detail in the article by Kohls et al.
70,000 cells per well is a lot of cells per well. We use between 500 and 2500 over a 72-hour period and then develop with MTS.
If your cells are slow-growing, you may want to wait a little longer to develop the assay, because the whole metabolism process is slowed. This is a weakness of the MTS system — you have to have a certain number of cells in the end in the control cells to get a decent reading on your plate reader.
In this case, you might want to try a more sensitive assay such as protein or DNA synthesis inhibition with incorporation of radiolabeled leucine or thymidine.
Q: Can you tell me how I would calculate the amount of a SAP-type targeted toxin that I might want to buy based on a desire to bilaterally kill cells of interest within a typical diffusion zone around an injection site in a rodent brain? Use CRF-SAP (Cat. #IT-13) as an example. Are we talking a few hundred dollars to run 40 animals or thousands of dollars?
A: For intraparenchymal application, usually 100 nanograms per injection site is too much; on the order of 5-10 nanograms is appropriate (for example: Lappi et al.)
So for CRF-SAP: at 10 nanograms per site, 20 nanograms per animal times 30 animals is 600 nanograms. Actual purchase price may vary. However, the average cost for this experiment using one vial of CRF-SAP in the 25-microgram size will run $8-$10 to treat all 30 animals. The CRF-SAP kit includes unconjugated saporin and a control immunotoxin; if you purchase that, the cost for the experiment described with 30 animals will be $12-$15.
Your question about how many injections are needed depends on the diffusion at the site of injection of the agent. Usually, peptide ligand toxins do not diffuse very far and in some cases (such as SSP-SAP, Cat. #IT-11) more than one injection is required. For the antibody targeted toxins, the antibody targeting agent is more resistant to tissue proteases and so there is a greater diffusion, though many researchers like to use several injections to completely cover an area. We’re not sure how big of an area you need or want to deplete; that would, of course, require a dosing regimen to determine.
Q: Will one injection permanently and reliably accomplish the deed?
A: One injection might or might not deplete the entire area that you are interested in; again, it depends on diffusion distance of the agent. However, those cells that are eliminated are eliminated permanently and will not come back. Plasticity to replace them is usually not seen.
Q: What are the typical criticisms (e.g., perhaps related to non-specific effects or interpretive difficulties) that the use of such products engender?
A: The typical reviewer requests demonstration of specificity and making a determination that, in fact, the proper cell type is hit and non-target cells are left intact is important.
Q: I purchased your secondary conjugate, Mab-ZAP (Cat. #IT-04). I am preparing to do a cytotoxicity assay and I’m wondering if my primary antibody should be sterilized prior to combining with Mab-ZAP?
A: Depending on the conditions of your lab in which you are using your antibody, it is possible that within a 72-hour period, you may see bacterial growth in your plates if the antibody was accidentally exposed to bacteria. It is recommended that, if you feel comfortable with the antibody, you can just go ahead and try it without sterilizing it, and if you do see bacterial growth, you can certainly filter sterilize the material through a 0.2 micron filter before using.
Q: I have a few questions about the Alexa488-labeled affinity-purified NGFr antibody (Cat. #AB-N43-FLA). Is it specific to extracellular p75? Can you use it on live cells? Does it work on fixed cells? Does it cause activation of the p75 receptor (i.e., result in apoptosis or changes in axon outgrowth in neuronal cells)?
A: This product does recognize extracellular p75 in both live and fixed cells. As for the activation, that’s an interesting question. There is no evidence of 192-IgG either causing apoptosis or neurite outgrowth as far as I can see. Chandler et al. (1984) report that the antibody “partially inhibits the regeneration of neurites from primed PC12 cells,” and it enhances NGF binding. But that’s about it, despite several studies being done with PC12 cells and in vivo. We assume all this holds upon treatment with 192-IgG-SAP (Cat. #IT-01) — until the cell dies from saporin poisoning.
Chandler CE, Parsons LM, Hosang M, Shooter EM (1984) A monoclonal antibody modulates the interaction of nerve growth factor with PC12 cells. J Biol Chem 259(11):6882-6889.
Q: Is there is any indication that intrastriatal administration of 192-IgG-SAP (Cat. #IT-01) will lesion the cholinergic neurons of the striatum. My sense from reviewing the literature is that these cholinergic neurons are not susceptible to the toxin, but I thought I’d ask to see if you had any information / experience regarding this point.
A: No, I don’t think it will work because the target of 192-IgG-SAP is p75, LNGFr, which is only expressed on the rat basal forebrain cholinergic neurons. Those striatal neurons don’t express p75 in the adult. The NK1r is often expressed in the striatum, and you can use SSP-SAP (Cat. #IT-11) for them, but that’s the best we can do right now.
Q: Your targeted toxin data sheet gives the following instruction for disposal: “Care in disposal is mandatory; autoclaving or exposure to 1 M sodium hydroxide will inactivate the material. All labware that comes into contact with this material should be likewise treated.” I am wondering if I can deactivate saporin by using 10% bleach or if everything has to be autoclaved?
A: Yes, you can use bleach to deactivate saporin prior to disposal or reuse of labware. If you are using nanogram quantities, these are too low to be toxic, so you can discard as you do your other non-hazardous laboratory materials without fear.
Q: Do conjugated toxins (dermorphin-saporin in particular) exhibit agonist effects? I’ve generated behavioral and tissue time course effects but have not established agonist effects for this conjugated toxin.
A: The peptide ligand toxins should exhibit agonist effects. They are constructed purposely to retain complete agonist activity, including for us the most important: internalization. So, for instance, SP-SAP (Cat. #IT-07) causes receptor internalization similar to SP, as reported in Mantyh et al.
As to dermorphin-SAP (Cat. #IT-12) specifically, it has agonist activity very much like dermorphin. This is reported in Porreca et al. in which it’s stated:
The bilateral microinjection of 3 pmol of dermorphin or of dermorphin-saporin directly into the RVM produced a robust antinociceptive effect in the 52°C hot-water tail-flick test. The peak antinociceptive effect of dermorphin, 78 ± 13.2% MPE, was not significantly different from that of the dermorphin-saporin conjugate, which was 59 ± 4.7% MPE (p > 0.5, Student’s t test).
Usually the amount needed to give a response is lower than the amount needed to kill a cell. Depending on what your system is; it may be a peculiarity of that system, but I would be a little concerned about not seeing an agonist effect. On the other hand, if you have demonstration of specific toxicity, it may not be all that crucial.